
WHAT IS TOTAL HIP REPLACEMENT (THR)?
Total Hip Replacement (THR), medically referred to as Total Hip Arthroplasty, stands as one of the most successful and life-changing surgical interventions in the history of modern orthopedics. For individuals suffering from the grueling effects of end-stage arthritis or traumatic joint injury, THR is not merely a medical procedure; it is a gateway to a pain-free life and a return to the activities they love.
At Physiotherapy Expert, we recognize that while the surgeon performs the mechanical repair, the ultimate success of the joint depends on the dedication to post-operative rehabilitation. Our mission is to bridge the gap between surgery and functional independence, ensuring that every patient navigates their recovery with confidence, strength, and expert clinical guidance. This guide provides an exhaustive look into the anatomy, surgery, and professional physiotherapy protocols required for a full recovery.
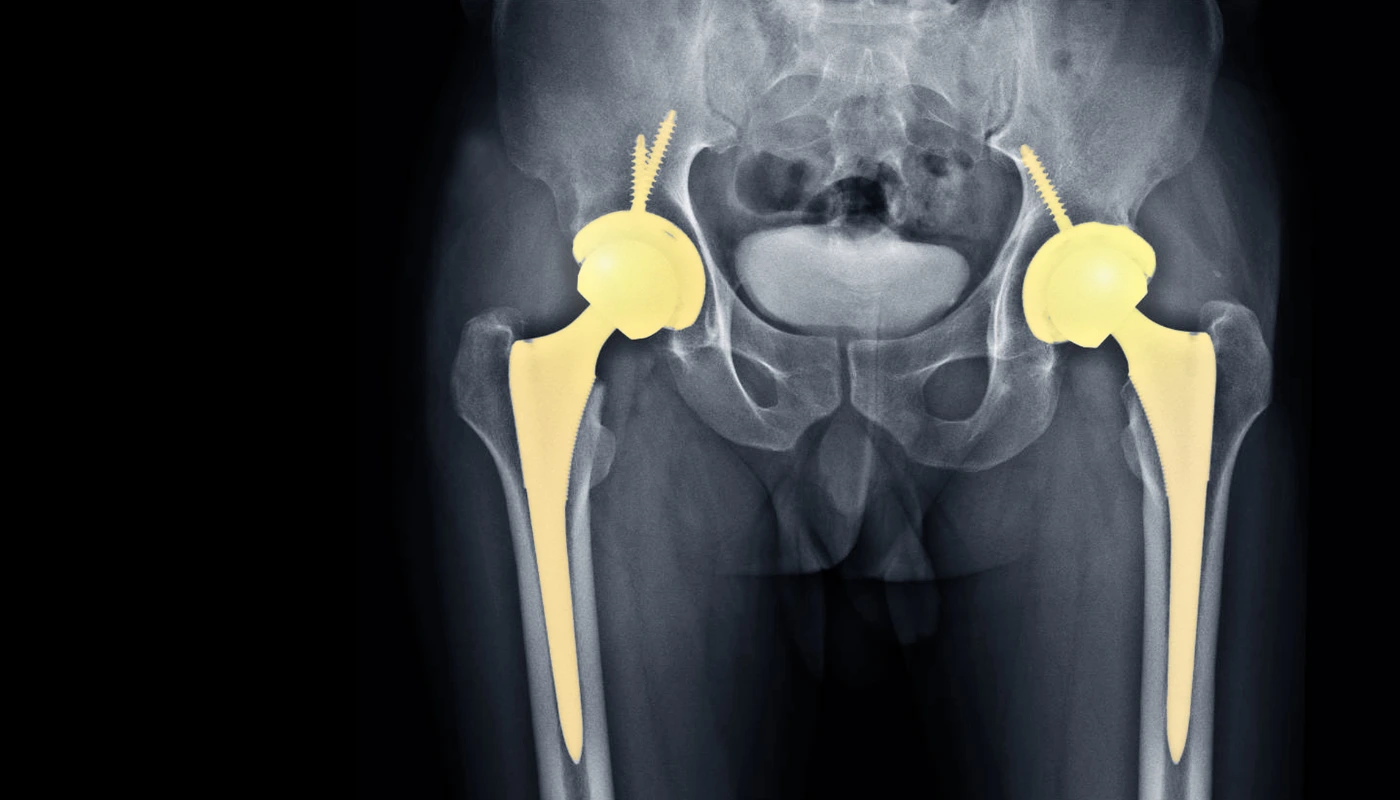
A Total Hip Replacement is a major reconstructive surgery where the damaged bone and cartilage of the hip joint are removed and replaced with prosthetic components. The hip is a “ball-and-socket” joint; in a healthy hip, the femoral head (the ball) rotates smoothly within the acetabulum (the socket) of the pelvis. When this joint becomes diseased or injured, the smooth cartilage that cushions the bones wears away, leading to a “bone-on-bone” environment.
During the THR procedure, the surgeon removes the arthritic femoral head and replaces it with a metal or ceramic ball attached to a stem that fits into the femur. The damaged socket is hollowed out and replaced with a metal shell, into which a durable plastic, ceramic, or metal liner is inserted. These new bearing surfaces allow for friction-free movement, mimicking the natural mechanics of a healthy human hip. At Physio Expert, we view the new joint as a high-performance tool that requires specific “tuning” through physiotherapy to reach its full potential.
SURGICAL TECHNIQUES AND ANATOMICAL APPROACHES
The path to recovery often begins with understanding the specific surgical approach utilized by your orthopedic team. The “approach” refers to the direction from which the surgeon accesses the hip joint, and this choice significantly influences early post-operative restrictions and muscle activation patterns.
The Posterior Approach
This remains the most traditional and widely used technique globally. The surgeon accesses the hip through the back of the joint, often involving a split in the gluteus maximus muscle. While it provides excellent visibility for complex cases, it historically carries a slightly higher risk of dislocation if “Hip Precautions” are not strictly followed. Patients must avoid bending the hip past 90 degrees, crossing their legs, or twisting their foot inward for the first six to twelve weeks to allow the posterior capsule to heal.
The Anterior Approach
Increasingly popular due to its “muscle-sparing” nature, the anterior approach accesses the joint from the front. Instead of cutting through major muscles, the surgeon works between the natural intervals of the muscles. The primary advantage is a potentially faster initial recovery and a lower risk of dislocation, as the posterior structures remain intact. From a physiotherapy perspective, these patients often reach early mobility milestones faster, though they still require intensive strengthening to stabilize the joint.
The Lateral Approach
This approach involves an incision on the side of the hip and usually requires the detachment of some of the hip abductor muscles (gluteus medius). While very stable, the rehabilitation focus for lateral approach patients is heavily weighted toward regaining abductor strength to prevent a permanent limp.
FIXATION METHODS: THE BIOLOGY OF STABILITY
One of the most critical aspects of THR is how the prosthetic components are secured to your natural bone. This is known as fixation, and it dictates how much weight you can safely put on your leg immediately after surgery.
Cemented Fixation
In a cemented hip replacement, a fast-drying bone cement (polymethylmethacrylate) is used to bond the prosthetic components to the bone. This method is often preferred for older patients or those with lower bone density, as it provides immediate, rock-solid stability. From a physiotherapy standpoint, cemented joints almost always allow for Immediate Full Weight Bearing. This means we can get you standing and walking with your full weight within hours of the procedure.
Cement-less (Porous) Fixation
Often referred to as “press-fit,” these implants have a rough, porous surface designed to mimic the structure of natural bone. Over time, your own bone grows into the pores of the metal, creating a permanent biological bond. This is the gold standard for younger, more active patients with high bone density. However, because the bond takes time to form, physiotherapists often prescribe “Touchdown Weight Bearing” or “Partial Weight Bearing” for the first six weeks to protect the implant while the bone integrates.
WHAT CAUSES THE NEED FOR TOTAL HIP REPLACEMENT?
The decision to undergo THR is usually the culmination of years of progressive pain and failed conservative treatments. The primary indications include:
- Osteoarthritis: The most common cause, where the “wear and tear” of aging destroys joint cartilage.
- Avascular Necrosis (AVN): A condition where the blood supply to the femoral head is interrupted, causing the bone to die and eventually collapse.
- Ankylosing Spondylitis and Rheumatoid Arthritis: Chronic inflammatory conditions that cause the body’s immune system to attack the joint lining.
- Developmental Dysplasia of the Hip (DDH): A condition present from birth where the hip socket is too shallow, leading to premature joint failure.
- Traumatic Fracture: In cases of severe hip fractures where the bone cannot be pinned, a replacement is the safest option.
PHYSIOTHERAPY TREATMENT AT PHYSIO EXPERT
Rehabilitation at Physiotherapy Expert is a structured, multi-phase journey. We don’t believe in a “one-size-fits-all” approach; instead, we follow a criteria-based progression that ensures you are safe at every step.
Phase 1: The Acute Protection Phase (0–4 Weeks Post-Op)
The primary goals in the first month are safety, pain management, and preventing complications.
- Cryotherapy: We use frequent cold therapy to manage the significant swelling that follows major orthopedic surgery.
- Circulatory Safety: Ankle pumps and early mobilization are critical to prevent Deep Vein Thrombosis (DVT).
- Hip Precautions Education: We spend intensive time teaching you how to move safely. This includes using a “reacher” to pick up items, using a raised toilet seat, and ensuring you do not cross your legs or twist your operated hip inward.
- Early Strengthening: Isometric exercises (squeezing the muscles without moving the joint) for the glutes, quads, and hamstrings to prevent further muscle wasting.
Phase 2: Functional Strengthening (4–8 Weeks Post-Op)
Once the initial surgical pain subsides and the incision has healed, we shift our focus to rebuilding the “engine” of the hip.
- Weight-Bearing Progression: Transitioning from a walker to a cane, ensuring that you do not develop a “Trendelenburg limp.”
- Closed-Chain Exercises: These are exercises where the foot is fixed on the ground, such as mini-squats and wall slides. These are more “functional” as they mimic real-life movements like sitting and standing.
- Pelvic Stability: We focus heavily on the gluteus medius. A stable pelvis is the foundation of a good walk.
- Balance Training: Using unstable surfaces (like foam pads) to retrain the nerves in your hip to communicate with your brain.
Phase 3: Advanced Mobility and Return to Life (8–12 Weeks Post-Op)
The final phase is about endurance and returning to the activities that make life worth living.
- Gait Refinement: Eliminating any lingering limp and ensuring your step length is equal on both sides.
- Cardiovascular Conditioning: Introduction of the stationary bike and longer walks.
- Resistance Training: Using resistance bands and light weights to build the power necessary for climbing stairs and hills.
- Sport-Specific Training: For our golfers, we work on rotational stability. For our hikers, we work on uneven terrain navigation.
THE PHYSIO EXPERT ADVANTAGE: OUR RECOVERY TOOLKIT
We utilize a variety of advanced modalities to accelerate your recovery:
- Neuromuscular Electrical Stimulation (NMES): Often, after surgery, the brain “shuts off” the quad muscles due to pain. We use NMES to provide an external electrical signal to force these muscles to contract, “re-teaching” them how to work.
- Thermotherapy: Before your exercise sessions, we may use heat to relax the surrounding soft tissues, making stretching more effective and comfortable.
- Laser Therapy: Low-level laser can be used to promote cellular repair near the incision site, reducing scar tissue density.
- Ultrasound: To manage deep-seated inflammation in the hip capsule during the later stages of rehab.
POTENTIAL COMPLICATIONS AND VIGILANCE
While THR is highly successful, it is still a major surgery. At Physio Expert, we are trained to monitor for:
- Joint Infection: We look for localized redness, warmth, or systemic fever.
- Deep Vein Thrombosis (DVT): We check for calf pain, redness, or excessive swelling below the knee.
- Dislocation: We continuously reinforce movement precautions to ensure the ball stays in the socket during the healing phase.
- Loosening: While rare with modern techniques, we monitor for “start-up” pain that could indicate the prosthesis is not settling correctly into the bone.
FREQUENTLY ASKED QUESTIONS
1. How long does the actual surgery take?
2. Is physiotherapy painful after a hip replacement?
3. When can I sleep on my side?
4. Can I go back to running or high-impact sports?
RELATED CONDITIONS TO MONITOR
- Hip Bursitis: Often, patients develop inflammation on the side of the hip as they change their walking patterns.
- Lower Back Pain: Years of limping before surgery often lead to stiff lumbar joints that require their own physiotherapy attention.
- Knee Pain: Because the hip and knee work as a chain, a new hip can sometimes temporarily change the stresses on the knee.


