
WHAT IS THE MEDIAN NERVE?
The Median Nerve is often referred to in clinical neurology as the “eye of the hand.” This title is well-earned, as the nerve provides the essential sensory feedback required for nearly every fine motor task we perform, from buttoning a delicate shirt to threading a needle or sensing the texture of a fabric. It is one of the three primary nerves of the upper limb, originating from the Brachial Plexus in the neck and traveling the entire length of the arm to reach the fingertips.
An injury to the median nerve is not merely a “numb hand”; it is a significant disruption of the human interface with the physical world. Without the median nerve, the thumb loses its ability to “oppose” the other fingers, effectively turning the hand into a flat, non-functional paddle. At Physiotherapy Expert, we specialize in the complex journey of nerve recovery. By utilizing the principles of Neural Plasticity and Axonal Regeneration, our specialized hand therapy programs aim to restore the bridge between the brain and the hand.
To understand the impact of an injury, one must first understand the nerve’s vast responsibilities. The Median Nerve is a “mixed nerve,” meaning it carries both motor signals (telling muscles to move) and sensory signals (carrying touch and pain data back to the brain).
1. Sensory Distribution
The median nerve provides sensation to the palmar surface (palm side) of the thumb, the index finger, the middle finger, and the radial half (thumb side) of the ring finger. It also covers the nail beds of these fingers on the back of the hand.
2. Motor Distribution
In the forearm, it controls the muscles that allow you to flex your wrist and pronate your arm (turn your palm down). In the hand, it controls the Thenar Muscles—the meaty bulge at the base of the thumb—which are responsible for “opposition,” the unique human ability to touch the thumb to the tips of the other fingers.
TYPES AND SITES OF MEDIAN NERVE LESIONS
The symptoms a patient experiences depend entirely on where the nerve is injured. At Physio Expert, we classify these injuries into “High” and “Low” lesions.
High Median Nerve Palsy (Above the Elbow)
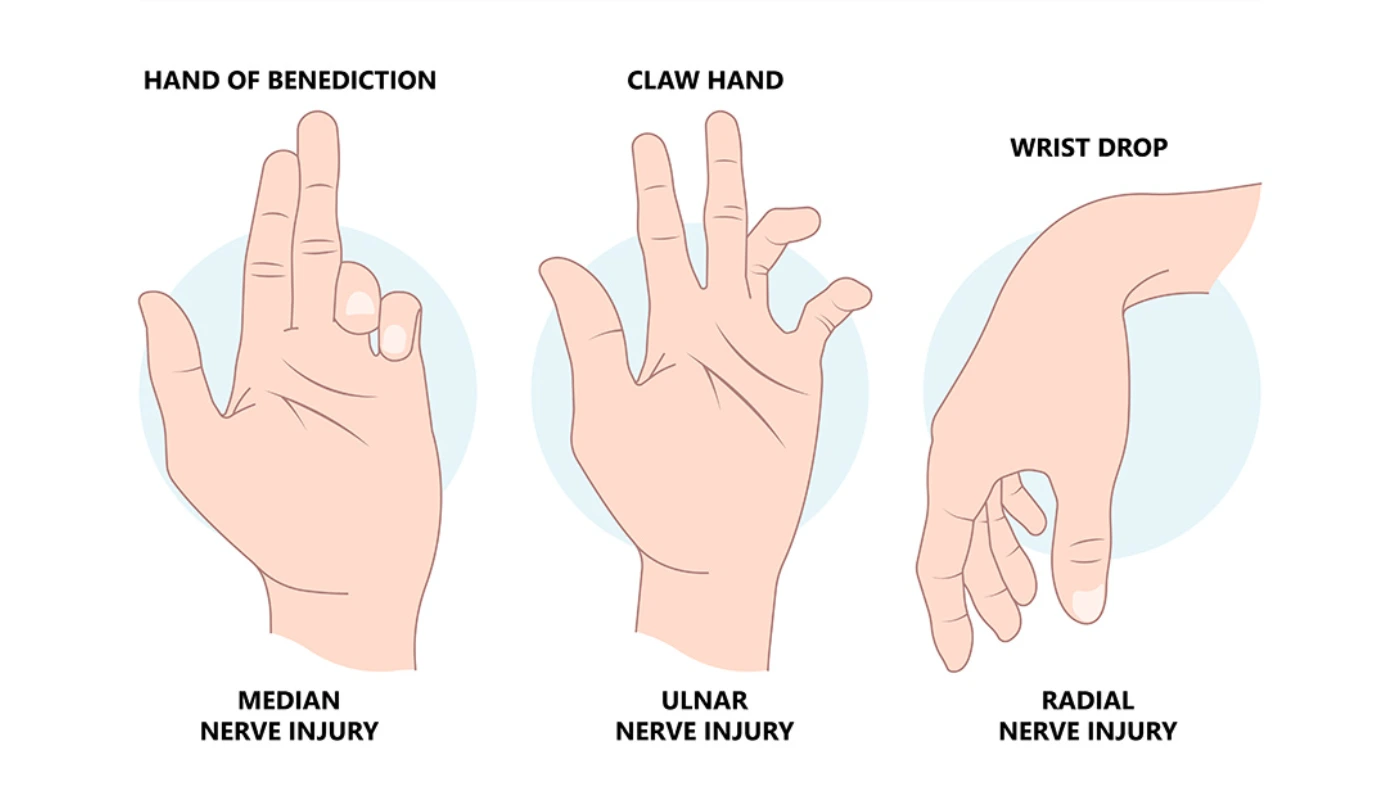
Injuries at this level are often caused by fractures of the humerus (upper arm bone) or compression in the forearm. A high lesion affects both the forearm muscles and the hand muscles. Patients with high lesions often display the “Hand of Benediction” when trying to make a fist—the thumb, index, and middle fingers stay straight because the deep flexor muscles are paralyzed.
Low Median Nerve Palsy (At the Wrist)
This is the most common form of injury, usually occurring within the Carpal Tunnel. Because the nerve has already sent its branches to the forearm muscles, a low lesion only affects the sensation in the fingers and the muscles of the thumb. This leads to “Ape Hand Deformity,” where the thumb falls into the same plane as the other fingers, losing its ability to stand out or oppose.
COMMON CAUSES OF MEDIAN NERVE DYSFUNCTION
Nerves are delicate structures, sensitive to pressure, stretching, and chemical changes. The most frequent causes of median nerve damage treated at our clinic include:
1. Carpal Tunnel Syndrome (CTS)
Chronic compression of the nerve within the narrow canal at the wrist. This is often due to repetitive strain, pregnancy, or inflammatory conditions like rheumatoid arthritis.
2. Pronator Teres Syndrome
The nerve becomes trapped as it passes through the two heads of the pronator teres muscle in the upper forearm. This is common in athletes or workers who perform repetitive gripping and twisting movements.
3. Traumatic Fractures
A “Supracondylar fracture” of the humerus (common in children) or a “Colles’ fracture” of the distal radius (common in adults after a fall) can stretch, bruise, or even sever the nerve.
4. Lacerations
Deep cuts to the wrist or forearm can partially or completely sever the nerve. These cases require surgical “Nerve Repair” or “Nerve Grafting” before physiotherapy can begin.
SYMPTOMS: RECOGNIZING NERVE DAMAGE
The median nerve provides clear “red flags” when it is under distress. If you notice any of the following, a neurological assessment is required:
1. Nocturnal Paresthesia: Numbness or “pins and needles” that wake you up at night, often relieved by “shaking out” the hand.
2. Thenar Atrophy: A visible flattening or hollowing out of the muscle at the base of the thumb.
3. The “Bottle Sign”: An inability to grip a round object (like a water bottle) firmly because the thumb cannot wrap around it.
4. Loss of Fine Motor Skills: Difficulty picking up coins, fastening buttons, or handwriting.
5. Pain in the Forearm: A deep, aching pain that may radiate up toward the shoulder.
DIAGNOSIS: CLINICAL AND ELECTRICAL PRECISION
At Physiotherapy Expert, we don’t guess—we assess. Our diagnostic process for nerve injuries includes:
1. Tinel’s Sign: We tap over the nerve at the wrist or elbow. A positive test results in an electric shock sensation in the fingers, indicating an irritated or regenerating nerve.
2. Phalen’s Test: You are asked to press the backs of your hands together for 60 seconds. If this triggers numbness, it confirms carpal tunnel compression.
3. Two-Point Discrimination: We use specialized tools to see if you can feel the difference between one point and two points on your fingertips, which measures sensory density.
4. Electromyography (EMG): We review electrical studies that measure how well your muscles are responding to the nerve’s signals.
PHYSIOTHERAPY TREATMENT: THE 12-WEEK NERVE RECOVERY ROADMAP
Nerve tissue is the slowest-healing tissue in the human body, growing at a rate of approximately 1mm per day (or 1 inch per month). Our 12-week protocol is designed to protect the nerve while encouraging this slow biological growth.
Phase 1: Protection and Nerve “Quietening” (Weeks 1–4)
1. Neutral Splinting: We provide custom-fitted splints to keep the wrist in a straight position, particularly at night. This maximizes the space in the carpal tunnel and allows blood flow to reach the nerve.
2. Edema Management: Using “Manual Lymphatic Drainage” to clear the fluid that often builds up around an injured nerve and increases pressure.
3. Tendon Gliding: Gentle exercises to keep the tendons from sticking to the nerve during the healing process.
Phase 2: Neural Mobilization and Desensitization (Weeks 4–8)
1. Nerve Flossing: These are specialized movements where we “pull” the nerve from one end while relaxing it at the other. This slides the nerve through its anatomical tunnels, preventing scar tissue from “tethering” the nerve.
2. Sensory Re-education: If the nerve is healing but the brain is “confused,” we use different textures (rough to smooth) to help the brain recognize touch signals again.
3. Scar Tissue Mobilization: If the injury was due to surgery or a cut, we use manual techniques to ensure the scar remains flexible.
Phase 3: Strengthening and Functional Mastery (Weeks 8–12)
1. Opposition Retraining: Using therapeutic putty to strengthen the thumb muscles.
2. Grip and Pinch Power: Progressive exercises to restore the ability to pinch (index to thumb) and power grip.
3. Ergonomic Correction: We analyze your workstation or athletic technique to ensure the injury does not return.
THE PHYSIO EXPERT ADVANTAGE: TECHNOLOGY FOR NERVE REPAIR
We integrate modern technology to give your nerves the best chance at recovery:
1. Neuromuscular Electrical Stimulation (NMES): We apply gentle currents to the thumb muscles to keep them “active” while the nerve is still growing down the arm.
2. Laser Therapy: Low-level cold laser therapy has been shown to increase cellular energy (ATP), which may help accelerate the rate of nerve fiber repair.
3. Biofeedback: Using visual sensors to help you see when you are successfully activating a weakened muscle.
SURGICAL INTERVENTION: WHEN IS IT NECESSARY?
Most median nerve compressions (like mild CTS) respond to physiotherapy. However, surgery (Carpal Tunnel Release or Nerve Decompression) may be necessary if:
1. There is constant, 24/7 numbness that does not change with position.
2. There is visible muscle wasting (Atrophy).
3. EMG tests show “Denervation,” meaning the muscle is no longer receiving any signals at all.
Post-surgical physiotherapy is vital to prevent the “Pillar Pain” and stiffness that can occur after nerve release surgery.
FREQUENTLY ASKED QUESTIONS
1. How long does it take for the numbness to go away?
2. Can I avoid surgery for Carpal Tunnel?
3. What happens if I ignore a Median Nerve injury?
4. Why does my thumb look flat?
RELATED CONDITIONS
Ulnar Nerve Palsy: Often confused with median nerve issues, but affects the pinky side of the hand.
Radial Nerve Injury: Leads to “Wrist Drop” and affects the back of the hand.
Thoracic Outlet Syndrome: Compression higher up in the shoulder that can mimic hand nerve pain.