
What Is Genu Varum?
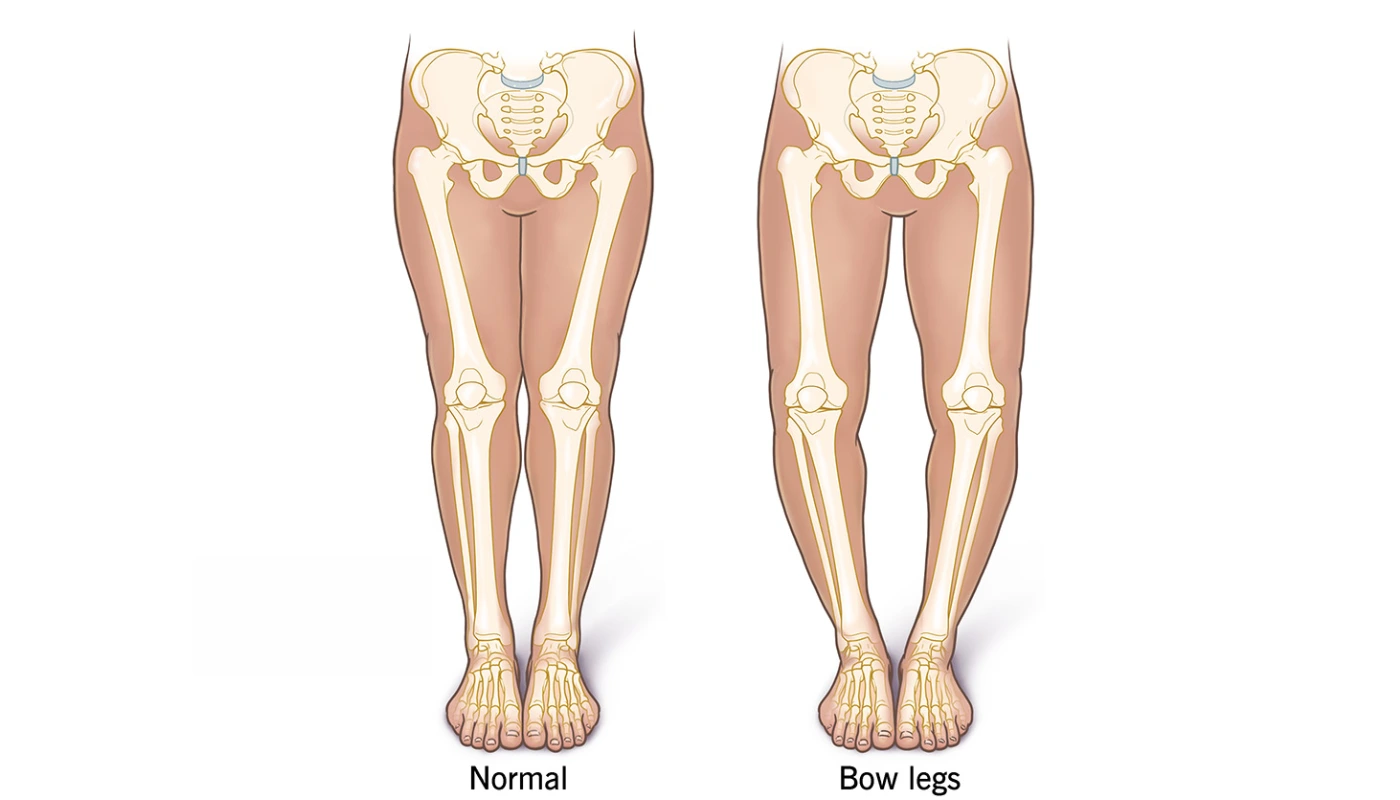
Genu Varum, commonly known as bow-leggedness, is a structural or functional physical deformity where the lower legs curve outward in relation to the thigh. When a person with Genu Varum stands with their feet and ankles touching, there is a distinct and measurable gap between the knees.
In the medical community, this is described as a varus deformity of the knee joint. While it is a normal developmental stage in infants (physiologic genu varum), it is considered pathological if it persists beyond the age of 3 or develops later in life due to injury, obesity, or degenerative diseases. At Physio Expert, we focus on correcting the biomechanical imbalances caused by this alignment to prevent long-term joint degradation.
The Anatomy of the “Varus” Angle
To understand Genu Varum, we look at the Q-angle and the mechanical axis of the leg. In a neutral leg, weight is distributed evenly across the medial (inner) and lateral (outer) compartments of the knee. In Genu Varum, the mechanical axis shifts inward, placing excessive compressive force on the medial compartment of the knee and stretching the lateral ligaments.
Classifications of Bow-Leggedness
- Physiologic Genu Varum: Normal bowing in children under 2 years old due to fetal positioning.
- Pathologic Genu Varum: Bowing that results from bone diseases like Rickets or Blount’s disease.
- Degenerative Genu Varum: Occurs in adults as the inner knee cartilage wears down (osteoarthritis), causing the leg to collapse outward.
- Traumatic Genu Varum: Resulting from malunion of fractures in the tibia or femur.
Signs and Symptoms of Genu Varum
While the most obvious sign is the physical “bowing” of the legs, Genu Varum often presents with several secondary symptoms that affect quality of life:
- Asymmetric Gait: An awkward walking pattern, often described as a “waddle,” where the patient shifts weight excessively to maintain balance.
- Medial Knee Pain: Pain localized to the inner side of the knee joint due to increased pressure.
- Lateral Ligament Strain: Tenderness on the outside of the knee where the ligaments are being overstretched.
- Toe-In Walking (Intoeing): Children with bow legs often walk with their toes pointed inward to compensate for the structural curve.
- Instability: A feeling that the knee might “give way” during physical activity.
- Reduced Range of Motion: Difficulty fully straightening or bending the knee without discomfort.
- Hip and Ankle Compensation: Pain in the hips or ankles as these joints try to compensate for the knee’s misalignment.
Causes and Risk Factors
The development of Genu Varum can be attributed to several factors, ranging from nutritional to mechanical:
1. Blount’s Disease
A growth disorder that affects the plates at the top of the shin bone (tibia). It can occur in toddlers or adolescents and causes the bone to grow abnormally.
2. Rickets (Vitamin D Deficiency)
A softening and weakening of bones in children, usually due to extreme and prolonged vitamin D, calcium, or phosphate deficiency. This makes the bones “pliable,” causing them to bow under the weight of the body.
3. Obesity
Excessive body weight places immense mechanical stress on the growth plates of the knees. In adults, obesity accelerates the wear of the medial meniscus, leading to a structural bow.
4. Bone Dysplasia
Genetic conditions that affect how bones and cartilage grow can lead to permanent Genu Varum.
5. Occupational Stress
Jobs that require heavy lifting or prolonged standing on hard surfaces can exacerbate a minor varus alignment into a symptomatic condition over time.
Pathology: The Biomechanical Breakdown
The pathology of Genu Varum involves a “vicious cycle” of mechanical loading. As the knee bows outward, the Medial Compartment of the knee undergoes excessive compression. This leads to:
- Meniscal Thinning: The inner shock absorber (medial meniscus) flattens.
- Cartilage Erosion: The protective coating of the bone wears away.
- Bone Spur Formation: The body creates extra bone (osteophytes) to try and stabilize the shifting joint.
- Ligament Laxity: The Lateral Collateral Ligament (LCL) becomes overstretched and “loose,” leading to joint instability.
Diagnosis at Physio Expert
We utilize a multi-step diagnostic process to determine if the bowing is structural (bone-based) or functional (muscle-based).
1. Physical Examination & Measurement
We measure the Intercondylar Distance—the gap between the knees when the ankles are touching. A gap wider than 2.5 inches in an adult usually requires intervention.
2. Gait Analysis
Using visual and digital tools, we observe the “loading response” of the foot and knee during walking. We look for a “lateral thrust,” where the knee juts outward during the stance phase.
3. Imaging (Radiographic Assessment)
- Full-Length Standing X-rays: This allows us to calculate the Mechanical Axis Deviation (MAD) from the hip to the ankle.
- MRI: Used to check for damage to the medial meniscus or cruciate ligaments caused by the bowing.
4. Blood Panels
To rule out metabolic causes like Rickets, we may suggest checking Vitamin D, Calcium, and Alkaline Phosphatase levels
Treatment Options
Medical and Surgical Intervention
- Bracing (Orthotics): Specialized knee braces (unloader braces) can help shift weight from the inner knee to the outer knee.
- Osteotomy: A surgical procedure where the tibia or femur is cut and realigned to straighten the leg.
- Growth Plate Stapling (Hemi-epiphysiodesis): In growing children, staples are placed on one side of the growth plate to “steer” the bone straight as it grows.
The Physio Expert 4-Phase Protocol for Genu Varum
Our physiotherapy approach focuses on balancing the muscle forces around the knee to stabilize the joint and prevent the need for surgery.
Phase 1: Pain Modulation & Inflammatory Control
- Electrophysical Agents: Using IFT (Interferential Therapy) and TENS to reduce medial knee pain.
- Cryotherapy: Applying cold packs to reduce inflammation after activity.
- Activity Modification: Identifying and pausing high-impact activities (like running on concrete) that aggravate the varus angle.
Phase 2: Correcting Muscle Imbalances
In Genu Varum, the outer muscles (Abductors) are often overworked, while the inner muscles (Adductors) and medial quadriceps (VMO) are weak.
- VMO Activation: Targeted exercises to strengthen the Vastus Medialis Obliquus to pull the kneecap inward.
- Hip Adductor Strengthening: Using squeeze balls and resisted cable work to bring the legs toward the midline.
- Myofascial Release: Deep tissue work on the Iliotibial (IT) Band and TFL, which are usually tight in bow-legged patients.
Phase 3: Functional Realignment & Proprioception
- Neuromuscular Electrical Stimulation (NMES): Using electrical pulses to “re-train” weak muscles to fire during walking.
- Single-Leg Balance: Training the brain to stabilize the knee on an unstable surface (Wobble boards).
- Gait Retraining: Teaching the patient to “engage” their core and glutes to prevent the knee from thrusting outward during each step.
Phase 4: Loading & Long-term Maintenance
- Squat Realignment: Performing squats with a focus on “knees over toes” tracking.
- Agility Drills: Controlled lateral movements to ensure the lateral ligaments can handle side-to-side stress.
- Home Exercise Program (HEP): A lifelong maintenance routine to keep the hip stabilizers strong.
Advanced Technology at Physio Expert
We don’t just use standard exercises; we employ advanced clinical technology:
- High-Frequency Ultrasound: To promote healing in the overstretched lateral ligaments.
- Pulsed Electromagnetic Field (PEMF): To stimulate bone and cartilage health in the compressed medial compartment.
- Laser Therapy: To reduce deep-seated inflammation within the joint capsule.
Patient Education: Protecting Your Knees
At Physio Expert, we believe an educated patient recovers faster. We teach you:
1. Proper Footwear
Avoid high heels or completely flat shoes. We often recommend lateral wedge insoles that slightly tilt the foot to offload the inner knee.
2. Weight Management
For every 1 kg of body weight lost, there is a 4 kg reduction in pressure on the knee joint per step.
3. Posture Awareness
Avoid “locking” your knees when standing. A “micro-bend” in the knees engages the muscles and protects the bone.
4. Environmental Modification
Using cushioned mats at home or work if you stand for long periods.
Related Conditions
- Genu Valgum (Knock Knees): The opposite of Genu Varum, where knees curve inward.
- Medial Compartment Osteoarthritis: The most common long-term result of untreated Genu Varum.
- Patellofemoral Pain Syndrome: Kneecap pain caused by poor tracking due to the bow.
- Pes Planus (Flat Feet): Often occurs as a compensatory mechanism for bow legs.