
WHAT IS GENU VALGUM?
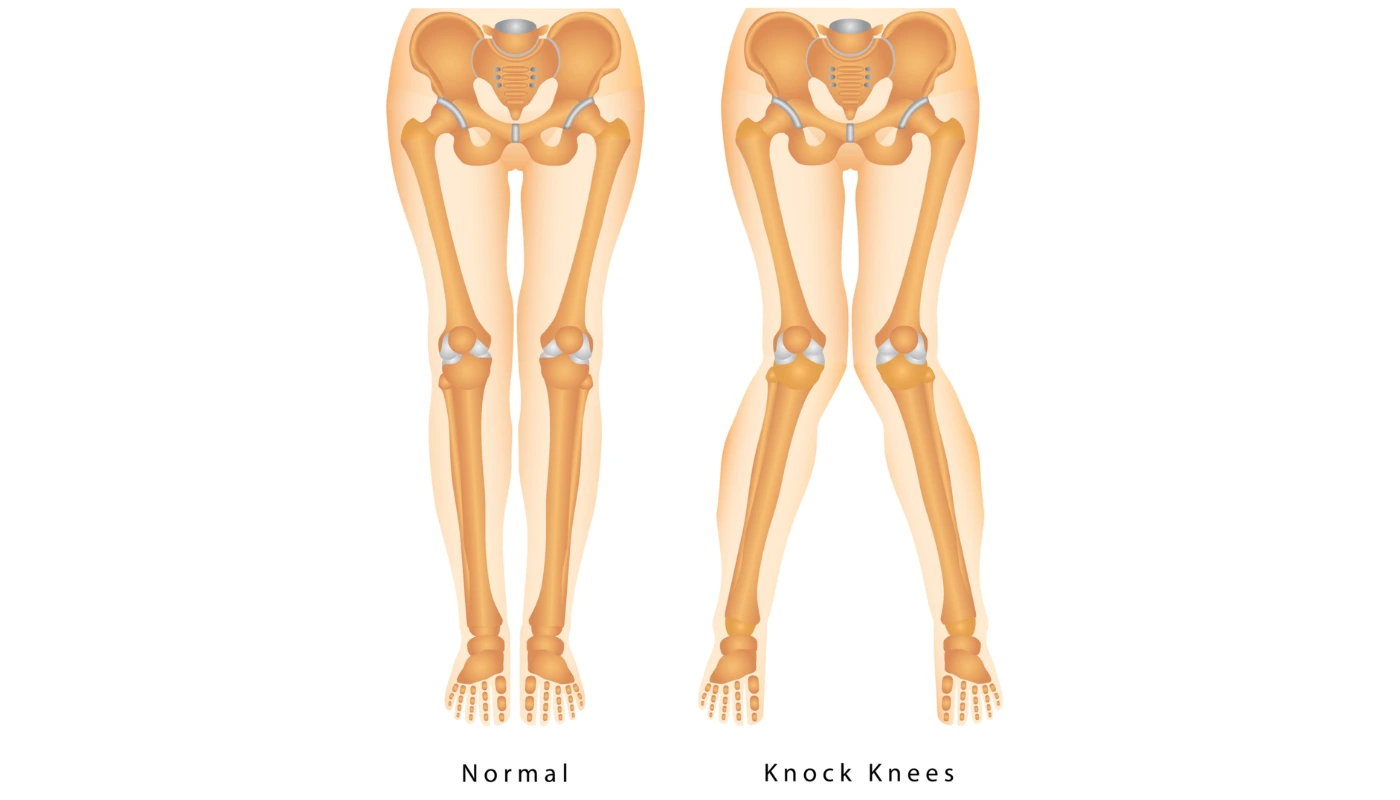
Genu Valgum, widely known as “knock knees,” is a common orthopedic lower limb deformity where the knees angle inward and touch each other when a person stands with their legs straightened. This inward tilt creates a significant gap between the medial malleoli (internal ankle bones) when the knees are in contact.
In clinical terms, “valgus” refers to a deformity where the distal (further) part of a joint is twisted outward away from the midline, while the joint itself points inward. At Physio Expert, we treat Genu Valgum not just as an aesthetic concern, but as a significant biomechanical misalignment that, if left unaddressed, can lead to premature joint wear, ligamentous laxity, and chronic pain in the hips and lower back.
The Developmental Timeline
It is essential to distinguish between Physiologic Genu Valgum and Pathologic Genu Valgum:
- Infancy (0–2 years): Most children are born with Genu Varum (bow legs).
- Early Childhood (2–4 years): Transition to Genu Valgum is a normal developmental stage.
- Stabilization (6–7 years): Most children’s legs naturally straighten. If the inward angling persists beyond age 7, or if it develops suddenly in adulthood, it is classified as pathological and requires professional intervention.
WHAT ARE THE CAUSES OF GENU VALGUM?
Genu Valgum is rarely caused by a single factor. It is typically the result of a complex interplay between bone structure, muscular balance, and external stressors.
1. Genetic Predisposition
Heredity plays a major role in the shape of the femoral neck and the alignment of the pelvis. If parents have a high “Q-angle” (the angle between the quadriceps and the patellar tendon), children are more likely to exhibit knock knees.
2. Growth Plate Injuries (Physeal Damage)
The growth plates at the end of the femur (thigh bone) and tibia (shin bone) are highly sensitive. An infection (osteomyelitis) or a fracture involving the lateral side of the growth plate can slow down growth on the outside while the inside continues to grow, forcing the knee inward.
3. Obesity and Mechanical Loading
Excessive body weight during formative years puts a “valgus stress” on the knees. To support the heavy load, the body shifts the center of gravity, often resulting in the collapse of the medial arches of the feet and the inward tilting of the knees.
4. Nutritional Deficiencies
Conditions like Rickets (Vitamin D deficiency) or Scurvy (Vitamin C deficiency) weaken the bone matrix. Soft bones are unable to support the body’s weight, leading to structural bending at the joints.
5. Underlying Medical Conditions
- Blount’s Disease: Though more common in Genu Varum, variations can cause valgus.
- Rheumatoid Arthritis: Chronic inflammation can erode the lateral compartment of the knee, causing the joint to collapse inward.
- Osteomalacia: The adult version of rickets, leading to bone softening.
WHAT ARE THE SYMPTOMS OF GENU VALGUM?
Beyond the visible “X-shape” of the legs, patients at Physio Expert often report:
- Medial Knee Pain: Pain located on the inside of the knee due to the stretching of the Medial Collateral Ligament (MCL).
- Lateral Compartment Compression: A “pinching” sensation on the outer side of the knee where the bones are pressing together.
- Anterior Knee Pain (PFPS): The kneecap (patella) does not track correctly in its groove, leading to “Runner’s Knee” symptoms.
- Circumduction Gait: To prevent the knees from “knocking” into each other while walking, the patient may swing their legs outward in a semi-circular motion.
- Foot and Ankle Issues: Most knock-kneed patients also suffer from Flat Feet (Pes Planus) and overpronation, as the inward collapse of the knee forces the arch of the foot to flatten.
- Lower Back Pain: An increased pelvic tilt to compensate for the leg alignment puts excessive strain on the lumbar spine.
PATHOLOGY: THE BIOMECHANICAL COLLAPSE
The pathology of Genu Valgum revolves around the Mechanical Axis. In a healthy leg, a straight line can be drawn from the center of the hip to the center of the ankle, passing directly through the middle of the knee.
In Genu Valgum, this line shifts laterally (outward). This creates a “long-lever” effect that:
- Compresses the Lateral Meniscus: The outer shock absorber is crushed, leading to early-onset osteoarthritis.
- Stretches the MCL: The inner ligament is constantly taut, leading to chronic instability.
- Alters Patellar Tracking: The quadriceps pull the kneecap toward the outside (the “J-sign”), which can lead to frequent patellar dislocations.
- Weakens the Hip Abductors: Because the knees are turned in, the Gluteus Medius becomes “long and weak,” further allowing the femur to rotate internally.
DIAGNOSTIC TESTS FOR GENU VALGUM
At Physio Expert, we utilize a multi-modal diagnostic approach to ensure the treatment plan is targeted.
1. Physical Examination & Intermalleolar Distance (IMD)
We measure the distance between the internal ankle bones while the knees are touching. An IMD greater than 8 cm is generally considered a clinical Genu Valgum.
2. Radiographic Imaging (X-rays)
Standing, full-length X-rays (teleroentgenogram) are essential. We measure the Hip-Knee-Ankle (HKA) angle. This tells us if the deformity is originating in the femur or the tibia.
3. MRI (Magnetic Resonance Imaging)
Used specifically if the patient reports sharp pain or “locking,” as this may indicate a lateral meniscus tear or cartilage damage caused by the valgus alignment.
4. Digital Gait Analysis
We use slow-motion video analysis to see how the knee behaves under dynamic load. This helps identify “Functional Genu Valgum,” which may only appear during running or jumping due to muscle weakness.
TREATMENT FOR GENU VALGUM
Non-Surgical Management
Most adolescent and adult cases are managed through specialized physiotherapy, bracing, and orthotics.
- Custom Orthotics: Medial arch supports can help “re-align” the kinetic chain from the ground up.
- Unloader Braces: These apply a counter-pressure to push the knee back toward a neutral alignment.
Surgical Intervention
Surgery is reserved for severe cases (HKA angle > 10 degrees) or when joint degeneration is imminent.
- Guided Growth (Hemi-epiphysiodesis): For children, a small plate is placed on the inner side of the growth plate to temporarily stop growth there while the outside catches up.
- Osteotomy: For adults, the bone is cut and realigned.
- Total Knee Arthroplasty (TKA): In elderly patients where Genu Valgum has led to end-stage arthritis.
PHYSIOTHERAPY TREATMENT AT PHYSIO EXPERT
Our rehabilitation program is divided into four focused phases to address both the symptoms and the root mechanical causes.
Phase 1: Pain Modulation & Inflammation Control
We use advanced electrotherapy to manage the acute pain caused by ligamentous stretch and joint compression.
- TENS & IFC: To block pain signals and reduce the “aching” sensation after walking.
- Thermotherapy: Heat packs are used to relax the tight lateral structures (IT Band and Lateral Hamstrings).
- Ultrasound Therapy: To promote healing in the strained medial collateral ligament.
Phase 2: Myofascial Release & Flexibility
In Genu Valgum, the outer structures are typically “tight/short” and the inner structures are “weak/long.”
- IT Band & TFL Release: Using manual therapy and foam rolling to reduce the outward pull on the knee.
- Adductor Stretching: Opening up the inner thigh to allow the femur to sit more neutrally.
- Lateral Hamstring Release: Addressing the tightness that contributes to the external rotation of the tibia.
Phase 3: Targeted Strengthening (The “Anti-Valgus” Routine)
This is the core of our treatment. We focus on the “Glute-Hip-Knee” connection.
- Gluteus Medius Strengthening: Using “clamshells” and “lateral monster walks” to prevent the femur from collapsing inward.
- VMO (Vastus Medialis) Activation: Strengthening the inner quad to ensure the kneecap stays in its groove.
- Hip External Rotator Training: To counter the internal rotation characteristic of knock knees.
- Short Foot Exercises: Strengthening the intrinsic muscles of the foot to rebuild the medial arch.
Phase 4: Proprioception & Dynamic Stability
We retrain the brain to keep the knees aligned during complex movements.
- Single-Leg Squats with Mirror Biofeedback: Ensuring the knee doesn’t “cave in” during the movement.
- Jump/Land Mechanics: Critical for athletes to prevent ACL tears, which are highly common in valgus-aligned individuals.
- Balance Board Training: Improving the reactive stability of the ankle and knee.
THE PHYSIO EXPERT ADVANTAGE: TECHNOLOGY
We go beyond simple exercises by utilizing:
- Neuromuscular Electrical Stimulation (NMES): We “force-fire” the gluteal muscles during walking to help the patient feel the correct alignment.
- Laser Therapy: To accelerate ATP production in damaged cartilage cells.
- Pulsed Electromagnetic Field (PEMF): To stimulate bone health in patients with nutritional or metabolic causes.
PATIENT EDUCATION & LIFESTYLE MODIFICATION
A successful recovery at Physio Expert involves a partnership with the patient.
1. Weight Management
Every extra pound of body weight adds 3–4 pounds of pressure to the knee joint. Maintaining a healthy BMI is the single best way to slow down the progression of Genu Valgum.
2. Footwear Education
Avoid “flat” sandals or worn-out sneakers. Look for shoes with a rigid heel counter and built-in arch support. We provide custom-molded insoles specifically for valgus correction.
3. Activity Choices
We recommend shifting from high-impact sports (basketball, long-distance running) to low-impact alternatives like swimming or cycling (with proper seat height) to protect the lateral meniscus.
4. Posture Correction
Avoid the “W-sitting” position (sitting on the floor with knees together and feet out to the sides), as this encourages internal femoral rotation and worsens the valgus angle.
RELATED CONDITIONS
Genu Valgum is often a precursor to or associated with:
- Patellar Dislocation: The lateral pull makes the kneecap prone to slipping out.
- ACL Tears: The “Valgus Stress” is the primary mechanism for non-contact ACL injuries.
- Pes Planus (Flat Feet): The primary foot deformity associated with knock knees.
- Hip Bursitis: Caused by the abnormal gait and pelvic tilt.