
What Is Flat Foot (Pes Planus)?
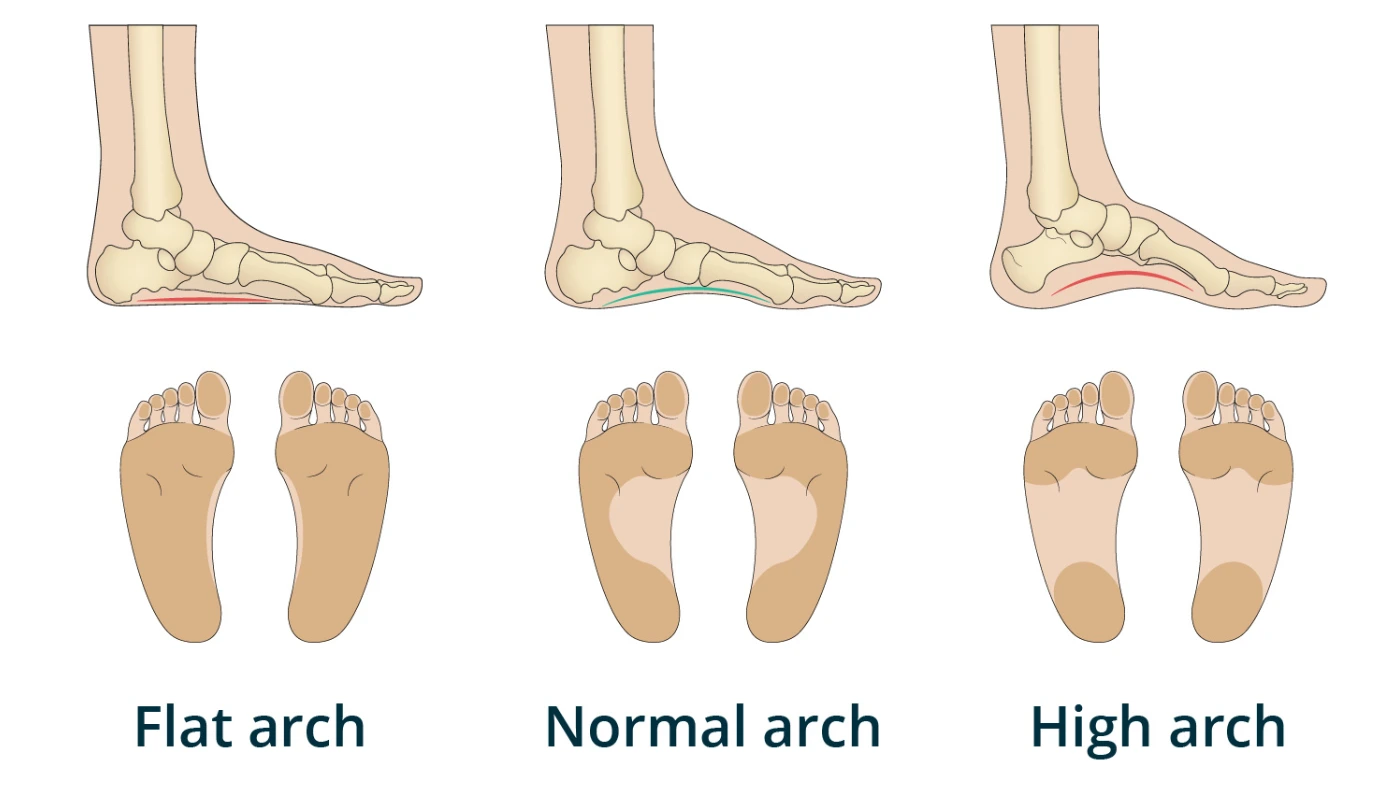
Flat Foot, clinically known as Pes Planus, is a common structural deformity where the longitudinal arches of the foot collapse, resulting in the entire sole making complete or near-complete contact with the ground. While often dismissed as a minor cosmetic issue or a simple variation of foot shape, the foot is actually the foundation of the entire human kinetic chain. A “flat” or unstable foundation can lead to a cascade of misalignments that travel upward, affecting the ankles, knees, hips, and even the lower back.
At Physiotherapy Expert, we view the foot as a dynamic, adaptable tripod. Our rehabilitation philosophy moves beyond simply “propping up” the arch with passive insoles. We focus on Intrinsic Foot Strengthening, Neuromuscular Re-education, and Functional Chain Alignment. This clinical guide explores the complex biomechanics of the arch, the various types of flat feet, and the professional physiotherapy protocols required to restore structural integrity and pain-free movement.
UNDERSTANDING THE ANATOMY OF THE ARCH
The human foot is an architectural marvel consisting of 26 bones, 33 joints, and over 100 muscles, tendons, and ligaments. These structures work in harmony to transform the foot from a flexible shock absorber at heel strike to a rigid lever for push-off. The primary structure responsible for the “spring” in our step is the Medial Longitudinal Arch.
The integrity of this arch is maintained by three distinct systems:
1. Bony Configuration: The wedge-shaped tarsal bones (specifically the navicular and cuneiforms) act as a “keystone” in an arch bridge, mechanically locking together under weight.
2. Ligamentous Support: The Spring Ligament and the Plantar Fascia act as high-tension cables, holding the bony segments together and preventing them from splaying apart.
3. Muscular Support (The Dynamic Stabilizers): The Posterior Tibial Tendon is the most critical muscle for arch height. It originates in the calf and attaches to the underside of the foot, literally “pulling” the arch upward during the walking cycle.
In a Flat Foot, one or more of these systems fail to provide sufficient tension. This causes the midfoot to “prime” or collapse toward the floor, a movement known as Overpronation.
TYPES OF FLAT FEET: FLEXIBLE VS. RIGID
At Physiotherapy Expert, our first diagnostic step is determining which category of Pes Planus you fall into. This distinction is vital because a flexible foot requires strengthening, while a rigid foot may require structural accommodation.
1. Flexible Flat Foot
This is the most common type. In these cases, a visible arch is present when the foot is non-weight-bearing (such as when sitting or dangling the legs). However, the moment the person stands up and applies weight, the arch disappears and the foot flattens. This is usually due to ligamentous laxity (loose ligaments) or weakness in the muscles that support the arch.
2. Rigid Flat Foot
In a rigid flat foot, the arch is absent regardless of whether the person is standing or sitting. The foot is stiff and does not “spring” back into shape. This is often caused by Tarsal Coalition (a congenital condition where two or more bones in the foot are fused together) or severe trauma that has altered the joint surfaces. Rigid flat feet often require specialized bracing or, in some cases, surgical consultation.
3. Adult-Acquired Flat Foot (PTTD)
This occurs when the Posterior Tibial Tendon—the primary arch supporter—becomes inflamed, stretched, or torn over time. As the tendon loses its functional strength, it can no longer hold the arch up, leading to a progressive and often painful collapse of the foot.
COMMON CAUSES AND RISK FACTORS
Flat feet can be a developmental trait from childhood or an acquired condition driven by lifestyle factors:
1. Genetics: Many individuals are born with naturally low arches or generalized ligamentous laxity (hypermobility). If your parents have flat feet, you are statistically more likely to develop them.
2. Footwear Habits: Prolonged use of shoes that lack arch support, or conversely, overly restrictive footwear that prevents the foot muscles from working, can lead to muscle atrophy.
3. Obesity: Excessive body weight puts a continuous mechanical strain on the spring ligament and the plantar fascia. Over time, this constant pressure causes these “cables” to stretch and sag.
4. Pregnancy: The hormone Relaxin is released to loosen the pelvic ligaments for childbirth, but it also affects the ligaments of the feet. Combined with a rapid increase in weight, many women find their shoe size increases due to a permanent drop in their arches.
5. Aging: Like any mechanical structure, the tendons and ligaments of the foot can wear down over decades, leading to “fallen arches” in later life.
SYMPTOMS: THE KINETIC CHAIN REACTION
A flat foot rarely stays a “foot problem” for long. Because the foot rolls inward (Overpronation), the lower leg must rotate internally to compensate. This rotation travels up the leg, affecting every joint along the way.
Common clinical symptoms addressed at Physio Expert include:
1. Foot and Arch Pain: A deep, aching sensation in the center of the foot or the heel.
2. Medial Ankle Swelling: Tenderness and puffiness along the inner ankle bone where the posterior tibial tendon is being overworked.
3. Shin Splints: Due to the repetitive tugging of the muscles on the shinbone as they struggle to stabilize the collapsing foot.
4. Knee and Hip Pain: Overpronation causes “Valgus” stress at the knee (knock-knees), which can lead to meniscus wear, ACL strain, or hip bursitis.
5. Lower Back Pain: An unstable foundation changes the tilt of the pelvis (anterior pelvic tilt), putting uneven pressure on the lumbar discs and facet joints.
DIAGNOSIS: THE PHYSIO EXPERT ASSESSMENT
We use a combination of physical tests and gait analysis to grade the severity of your flat foot and its impact on your movement:
1. The “Wet Foot” Test: We analyze the footprint to see the surface area of contact. A total footprint indicates a Grade 3 flat foot.
2. The “Too-Many-Toes” Sign: When viewed from behind, if the heel rolls out (valgus), more toes are visible on the outside of the foot than is normal.
3. Single-Leg Heel Raise: We ask you to stand on one leg and go up on your tiptoes. If the heel does not “invert” (tilt inward), it is a clear sign that the posterior tibial tendon is failing to support the arch.
4. Digital Gait Analysis: We observe your walking and running cycle on a treadmill to see exactly when the arch collapses—whether it happens at initial contact or during the push-off phase.
PHYSIOTHERAPY TREATMENT: THE 12-WEEK RECONSTRUCTION
The goal at Physiotherapy Expert is to build a “Functional Arch.” While we may not change the bone shape of an adult foot, we can give the foot the muscular strength to support itself without relying entirely on external props.
Phase 1: Pain Relief & Mobility (Weeks 1–4)
1. Myofascial Release: Releasing the tight calf muscles (Gastroc/Soleus) and the Plantar Fascia. Tight calves act like a “bowstring,” pulling the foot into a flat position.
2. Joint Mobilization: Restoring movement to the “stiff” joints of the midfoot and ankle. If the ankle joint is stiff, the foot is forced to collapse to find movement.
3. Kinesiology Taping: We use specific taping patterns to provide a “tactile lift” to the arch, giving the brain constant sensory feedback on where the arch should be.
Phase 2: Intrinsic Muscle Activation (Weeks 4–8)
1. Short Foot Exercise (The Arch Lift): This is the most important exercise in our protocol. We teach you how to pull the ball of your foot toward your heel without curling your toes, effectively “shortening” the foot and lifting the arch.
2. Toe Yoga: Learning to lift the big toe independently of the four smaller toes. This strengthens the Abductor Hallucis, the primary muscle of the medial arch.
3. Towel Curls: Using the toes to scrunch up a towel, which builds the small, deep muscles in the sole of the foot.
Phase 3: Global Integration & Stability (Weeks 8–12)
1. Proprioceptive Training: Standing on one leg on unstable surfaces (like foam pads or BOSU balls). This forces the foot to rapidly stabilize the entire body, building “reflexive” arch support.
2. Functional Squatting: Ensuring the knee and hip stay aligned while the foot maintains its arch under the weight of the body.
3. Plyometric Drills: Controlled hopping and jumping to ensure the arch can handle the high impact of running and jumping in sports.
THE ROLE OF ORTHOTICS: SUPPORT VS. CRUTCH
At Physiotherapy Expert, we believe orthotics (insoles) should be a “bridge,” not a “permanent crutch” for most flexible flat feet.
A. Custom Orthotics: For rigid cases or severe PTTD, custom-molded inserts can redistribute pressure and prevent the deformity from worsening.
B. Temporary Support: We often use “off-the-shelf” orthotics in the first few weeks of rehab to reduce pain, allowing you to perform your strengthening exercises more effectively.
C. The Exit Strategy: As your foot gets stronger, we aim to gradually reduce the “aggressive” nature of the support, allowing your foot to do the work it was biologically designed to do.
THE PHYSIO EXPERT ADVANTAGE: TECHNOLOGY FOR THE FEET
We supplement our hands-on care with modern medical technology:
Laser Therapy: To reduce inflammation in the posterior tibial tendon or the plantar fascia during the acute phase.
Neuromuscular Electrical Stimulation (NMES): We use small electrodes to help you “feel” and activate the muscles of the arch that may have been “dormant” for years.
Video Analysis: Providing you with a visual “before and after” of your walking mechanics so you can see the progress in your arch control.
FREQUENTLY ASKED QUESTIONS
1. Is having flat feet a disability?
2. Can I “cure” my flat feet with exercise?
3. Why do my flat feet cause back pain?
4. Should my child wear orthopedic shoes?
RELATED CONDITIONS
Plantar Fasciitis: Chronic heel pain caused by the constant stretching of the sole due to a collapsed arch.
Bunions (Hallux Valgus): Flat feet increase the pressure on the big toe joint, often leading to the development of bunions.
Achilles Tendonitis: Overpronation puts an uneven “twist” on the Achilles tendon, leading to inflammation and pain.