
What Is Disc Bulge?
A Disc Bulge, often colloquially referred to as a “slipped disc” or “protruding disc,” is one of the most common yet misunderstood spinal conditions treated in modern orthopedics. While the diagnosis can sound daunting, a disc bulge is often a manageable mechanical issue that responds exceptionally well to structured, evidence-based physiotherapy. At Physiotherapy Expert, we view the spine not as a fragile stack of bones, but as a dynamic, resilient system capable of healing and adaptation.
Our approach to disc bulge recovery moves beyond simple pain relief. We focus on Spinal Decompression, Biomechanical Correction, and Neuromuscular Re-education. This comprehensive guide provides a 2200-word deep dive into the anatomy, pathology, and professional rehabilitation strategies required to transform a debilitating spinal injury into a foundation for long-term strength.
UNDERSTANDING THE ANATOMY OF THE INTERVERTEBRAL DISC
To understand a bulge, one must first understand the “shock absorbers” of the human body. The intervertebral disc is a sophisticated structure located between each vertebra in the spinal column. It serves three primary functions: acting as a shock absorber, allowing for multi-directional spinal flexibility, and maintaining the height of the neural foramina (the exit doors for your nerves).
The disc consists of two main components:
1. The Nucleus Pulposus: This is the soft, jelly-like inner core. It is composed mostly of water and collagen fibers, providing the hydraulic resistance needed to handle vertical loads.
2. The Annulus Fibrosus: This is the tough, multilayered outer ring made of strong fibrocartilage. It acts like a radial tire, encasing the nucleus and keeping it centered under pressure.
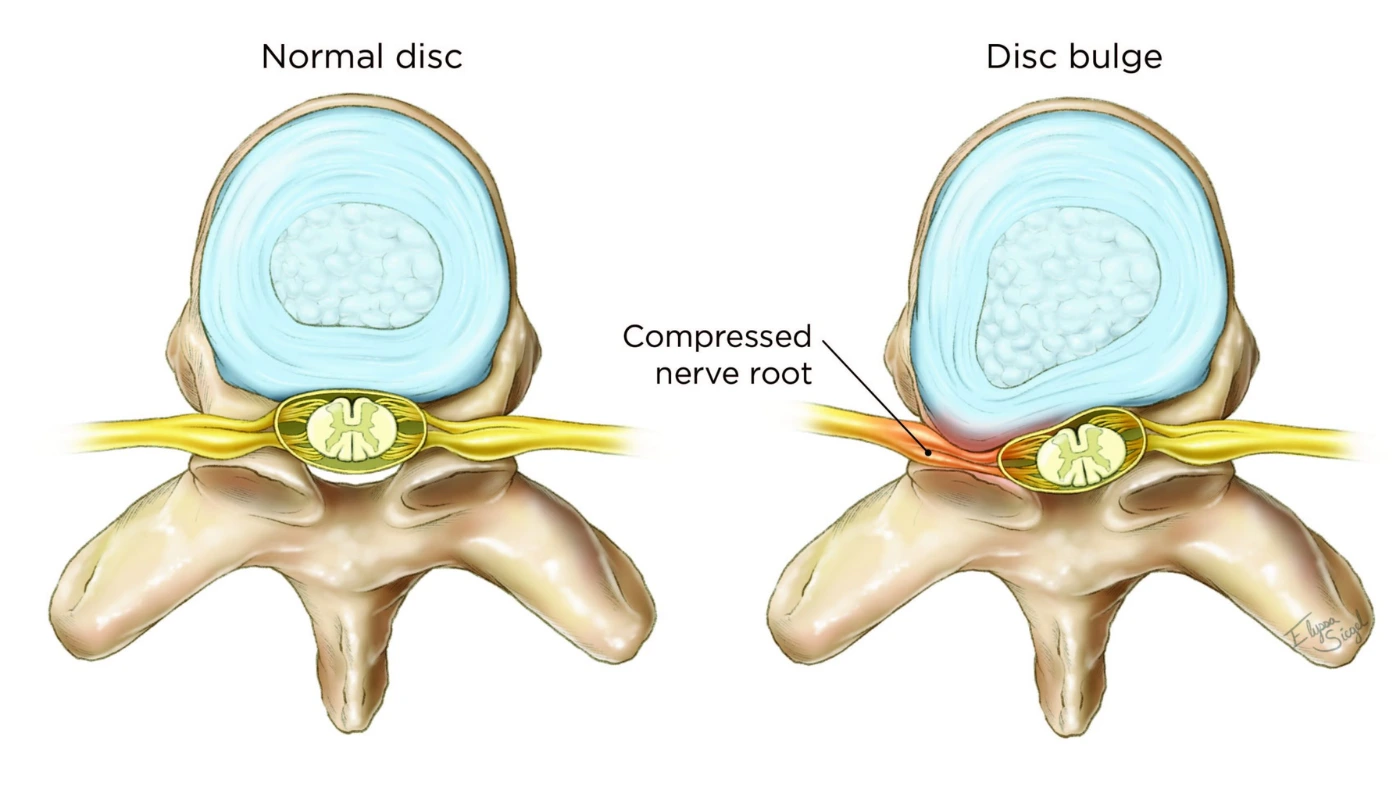
A Disc Bulge occurs when the tough outer layers of the annulus are stretched or weakened, allowing the soft nucleus to “bulge” outward. Unlike a herniation, where the jelly actually leaks out through a tear, a bulge is a change in the shape of the disc that can still put significant pressure on the spinal cord or exiting nerve roots.
THE STAGES OF DISC DEGENERATION
At Physiotherapy Expert, we use specific clinical terminology to describe the severity of your condition based on imaging (MRI or CT scans):
Stage 1 (Degeneration): Chemical changes associated with aging cause the discs to weaken, but without a significant bulge.
Stage 2 (Prolapse (Bulge)): The shape of the disc changes, creating a visible protrusion into the spinal canal.
Stage 3 (Extrusion (Herniation)): The nuclear jelly breaks through the wall of the annulus but remains attached to the disc.
Stage 4 (Sequestration): The nuclear material breaks off entirely and moves into the spinal canal.
Understanding which stage you are in is vital for determining the “load tolerance” of your spine during physiotherapy.
COMMON CAUSES AND RISK FACTORS
A disc does not bulge without reason. It is typically the result of Cumulative Micro-trauma or an acute Macro-trauma.
1. Poor Biomechanics and Lifting Techniques
Lifting a heavy object with a rounded back (spinal flexion) puts immense “shear force” on the posterior part of the disc. Over time, these repetitive stresses create microscopic tears in the annulus.
2. Sedentary Lifestyle and “Sitting Disease”
Prolonged sitting increases the intradiscal pressure by up to 40% compared to standing. When we sit with a slumped posture, the front of the vertebrae pinch the disc, forcing the nucleus to migrate backward—where the nerves live.
3. Degenerative Disc Disease (DDD)
As we age, our discs naturally lose water content (desiccation). A “dry” disc is less flexible and more prone to cracking or bulging under normal daily loads.
4. Genetics and Body Weight
Some individuals possess a genetic predisposition to weaker collagen structures. Additionally, carrying excess body weight puts a constant, 24/7 compressive load on the lumbar discs, accelerating wear and tear.
SYMPTOMS: BEYOND BACK PAIN
A disc bulge in the lower back (Lumbar) or neck (Cervical) presents a variety of symptoms depending on which nerve is being “pinched.”
A) Sciatica: Sharp, electric-like pain that travels from the lower back, through the buttock, and down the leg to the foot.
B) Radiculopathy: Numbness, tingling (“pins and needles”), or a “cold” sensation in a specific patch of skin.
C) Muscle Weakness: Difficulty standing on your toes or heels, or a loss of grip strength in cervical cases.
D) The “Antalgic Lean”: Many patients walk with a tilt to one side. This is the body’s involuntary attempt to shift the spine away from the bulging disc material.
E) Increased Pain with Coughing or Sneezing: These actions increase “Valsalva pressure” inside the spine, which temporarily pushes the bulge harder against the nerve.
DIAGNOSIS: THE CLINICAL BLUEPRINT
At Physiotherapy Expert, we combine physical provocation tests with advanced imaging to build your recovery plan:
1. Straight Leg Raise (SLR) Test: While lying on your back, we gently lift your leg. If you feel sharp pain below the knee between 30 and 70 degrees, it is a hallmark sign of a lumbar disc bulge.
2. Slump Test: A more sensitive neural tension test performed while sitting to determine if the nerves are “tethered” by the bulge.
3. Manual Muscle Testing: We check for “myotomal” weakness to pinpoint exactly which spinal level (e.g., L4, L5, or S1) is affected.
4. MRI Review: While we treat the person and not the scan, an MRI helps us visualize the direction of the bulge (Central, Posterolateral, or Foraminal), which dictates our exercise selection.
PHYSIOTHERAPY TREATMENT AT PHYSIO EXPERT: THE 12-WEEK ROADMAP
Nerve tissue is highly sensitive to pressure. Our rehabilitation protocol is designed to “centralize” your pain—moving it from your leg back to your lower back—and eventually eliminating it entirely.
Phase 1: Acute Decompression & Symptom Management (Weeks 1–4)
The goal is to reduce inflammation and create “space” for the nerve.
A) Directional Preference (McKenzie Method): We find the specific movement (usually spinal extension) that “pushes” the bulge back toward the center of the disc.
B) Manual Traction: Our therapists use hands-on techniques to gently pull the vertebrae apart, creating a “vacuum effect” that can help retract the bulge.
C) Cryotherapy: Using medical-grade cold packs to reduce the chemical inflammation around the nerve root.
D) Nerve Flossing: Gentle gliding exercises to ensure the nerve doesn’t get stuck in scar tissue.
Phase 2: Core Stabilization & “The Inner Corset” (Weeks 4–8)
Once the sharp pain is managed, we must stabilize the segment to prevent a relapse.
A) Activation of the Transverse Abdominis: Teaching you how to engage the deep abdominal wall to increase intra-abdominal pressure, which supports the discs from the front.
B) Multifidus Strengthening: Building the tiny muscles that sit directly on the vertebrae to provide “segmental” stability.
C) Pelvic Tilt Correction: Balancing the hip flexors and hamstrings to ensure the pelvis sits in a “neutral” position, reducing the load on the lower discs.
Phase 3: Functional Loading & Resilience (Weeks 8–12)
In the final phase, we prepare you for the demands of real life.
A) Hip Hinge Mastery: Training you how to bend and lift using your hips rather than your spine.
B) Progressive Weight Training: Controlled deadlifts and carries (with strict form) to build a “muscular armor” around your spine.
C) Proprioceptive Training: Using unstable surfaces to sharpen the brain’s ability to protect the spine during sudden movements.
THE PHYSIO EXPERT ADVANTAGE: TECHNOLOGY IN SPINAL REHAB
We utilize modern tools to accelerate the biological healing of the disc:
Laser Therapy: Low-level laser can penetrate deep into spinal tissues, stimulating ATP production and accelerating the repair of the annular fibers.
Neuromuscular Electrical Stimulation (NMES): To “re-wake” core muscles that have been “shut off” by the brain due to chronic pain.
Kinesiology Taping: Providing a 24/7 “tactile reminder” to maintain a neutral, safe posture.
LIFESTYLE AND ERGONOMIC INTEGRATION
Recovery doesn’t end when you leave the clinic. We help you modify your environment:
The “Sitting Break”: We implement the 20/20/20 rule—every 20 minutes, stand for 20 seconds and perform 20 pelvic tilts.
Lumbar Support: Ensuring your office chair and car seat maintain the natural “Lordosis” (curve) of your lower back.
Sleep Posture: Advising on pillow placement (between the knees for side sleepers) to keep the spine neutral overnight.
FREQUENTLY ASKED QUESTIONS
1. Does a disc bulge always require surgery?
2. How long does it take for a disc bulge to heal?
3. Can I still exercise with a disc bulge?
4. Why is my pain worse in the morning?
Related Conditions
Spinal Stenosis: A narrowing of the spinal canal, often worsened by a disc bulge.
Spondylolisthesis: The slipping of one vertebra over another.
Piriformis Syndrome: A condition where a muscle in the buttock mimics the symptoms of a disc-related sciatica.